

New York is living through a tale of two vaccine rollouts. In early February, New York City released data showing that eligible Black and Latino populations are receiving a smaller percentage of vaccine doses than white residents, a pattern echoed elsewhere in the state. The same applies across the nation, where Black and Latino populations also account for a smaller portion of vaccinations than their share of coronavirus cases and deaths.
“The fact that we don’t have real-time data to adjust our strategies is very distressing,” says Kirsten Bibbins-Domingo, professor and chair of the department of epidemiology and biostatistics at the University of California San Francisco.
These tensions are magnified as new companies seek emergency authorization for their vaccines. So far, some up-and-comers in the second wave of candidates haven’t yielded the same level of protection as the mRNA vaccines from Pfizer and Moderna.
On Wednesday, the FDA reported the one-dose candidate from Johnson & Johnson is 72 percent effective at preventing moderate to severe cases of COVID-19 in regions without the variants. For the mRNA vaccines by Pfizer and Moderna, this protection was upwards of 90 percent in clinical trials. The latter pair also generate more antibodies, a larger percentage of recipients with immunity defenses called T-cells, and higher efficacy among older adults and people with pre-existing conditions than Johnson & Johnson.
Moreover, the Johnson & Johnson vaccine prevented 60 to 70% of asymptomatic infections, a proxy for stopping the spread of the virus. Multiple large-scale studies in Israel, where the vaccine campaign has thrived, suggest two doses of Pfizer’s vaccine can block coronavirus transmission at a higher rate. The latest involving nearly 600,000 recipients, published Wednesday in the New England Journal of Medicine, showed one shot of Pfizer offers 60% effectiveness, while two doses protect 92% of the time.
These differences raise ethical questions around the next stages of the vaccine rollout.
If certain demographics have fallen behind, then policymakers must now wrestle with who should get the more effective mRNA vaccines, which require super-cold temperatures and two shots. The Johnson & Johnson vaccine may be less effective at preventing symptoms and transmission, but only requires one dose and can be stored in normal refrigerators—so it is more likely to be used in under-resourced settings. Johnson & Johnson did not respond to a request for comment.
Illustration of SARS-COV-2 virus particles. Note: not to scale.
National Institute of Allergy and Infectious Diseases, NIHThe Pros And Cons Of Less Efficacy
Mathematically speaking, the best way to control the pandemic would be to inoculate as many people as possible as fast as we can with any vaccine above 60% efficacy.
“Our models have shown that vaccinating more people faster is better than waiting for a vaccine with a higher efficacy,” says Bruce Y. Lee, a professor of health policy and management at CUNY and the director of the group Public Health Informatics, Computational, and Operation Research (PHICOR). Six other medical professionals interviewed for this article also recommended getting any vaccine that becomes available.
Overly focusing on infection rates may also downplay one of the largest benefits of all three vaccines, says Stella Safo, the co-founder of VoteHealth 2020 and an HIV primary-care provider at the Icahn School of Medicine at Mount Sinai. She says, “The message we should be conveying is they all did a good job in preventing serious infection and death.” That’s why some experts suggest the U.S. should now follow the UK in delaying the second dose of mRNA vaccines, helping stretch limited supplies.
But a weaker vaccine regimen will prevent less illness than a stronger one—something worth considering given chronic COVID. It’s also unclear how long immunity from any of the vaccines will last, especially now that immunity-dodging variants are arising.
“If one dose [of the mRNA vaccines] proves less effective, it ultimately may undermine trust,” warns Justin Feldman, a fellow at the Francois-Xavier Bagnoud Center for Health and Human Rights at Harvard University. Plus, the Biden administration has just purchased millions of additional doses from both Pfizer and Moderna, so supplies at local sites will soon increase to cover second shots.
If vaccines do indeed reduce transmission, as preliminary studies suggest, there’s also a strong argument to shift vaccinations to younger populations, who play a larger role in spreading the virus.
“That would further emphasize the need to focus on essential workers, who tend to be younger people of color,” Feldman says.
Vaccines with lower efficacy might also call for more frequent booster shots—at a time when cities and states are already struggling to convince at-risk groups and some staff in health care settings and nursing homes to take two shots. Deliver too many weaker vaccines in one area, and its recovery will be slower than those with access to the best vaccines.
There is also the justified mistrust in the medical system in many BIPOC communities, Safo explains, “given not even historical examples of abuse in medicine, but current experiences, when they got to the ER or the doctor and are treated differently.”
Overcorrecting For Disparities—And Variants
Minority groups have received fewer doses of COVID-19 vaccines, but the reasons might surprise onlookers.
Kaiser Family Foundation conducted a nationwide survey of those who want to “wait and see” with these life-saving drugs. They found Black and Hispanic adults are actually more responsive to pro-vaccine messages than white adults who are hesitant. And information gaps are feeding the reluctance among Black and Hispanic communities, who are more likely to be worried about side effects.
For Safo, access to supplies is also a huge problem—and one that must be addressed first. Some communities—especially older ones—lack the technology required to find an online appointment and the transportation to reach vaccine hubs. Although COVID-19 vaccines are free, many states ask for insurance information to make an appointment—deterring those worried about costs or legal documentation.
“If you aren’t giving people a chance to say no, how can you attribute lower rates to hesitancy?” asks Jewel Mullen, associate dean for health equity at the University of Texas at Austin Dell Medical School.
If you aren’t giving people a chance to say no, how can you attribute lower rates to hesitancy?
Mullen was on the National Academies of Science, Engineering, and Medicine committee that created guidelines for equitable vaccine distribution. She explains they decided to use the Centers for Disease Control and Prevention’s social vulnerability index, instead of race and ethnicity—and not just to avoid anti-discrimination legal challenges. More so than race, it's the social determinants of health—things like living and working conditions—that raise the risk of contracting COVID-19, as well as the likelihood of having comorbidities, like diabetes, that elevate the risk of severe illness.
Safo says, “If those track with certain race and ethnic groups, and they’re not over-corrected for [in the vaccine rollout], the system perpetuates these disparities.”
That’s one reason why Uché Blackstock, founder and CEO of Advancing Health Equity in New York City and Yahoo medical contributor, is advocating for eliminating age considerations for Black Americans who want to get the vaccine. “If you give priority over a certain age, you’re actually prioritizing white lives, and ignoring the historical and current structural inequities that shorten Black lives,” she says.
New York is belatedly attempting to address these equity concerns by reserving initial appointments at six new state-run vaccination sites for residents of underserved zip codes. They are reserving appointments for walk-ins, so people who may have trouble navigating online systems or have unpredictable schedules can more easily get in. Mullen says strengthening ties with trusted stakeholders, like religious leaders, and building more effective partnerships with community organizations will help increase vaccine access and decrease misinformation.
“Messengers matter,” Safo says, explaining she is helping train clinicians of color to do outreach.
Here And Everywhere
Equity concerns get even more complicated when considering the global challenge at hand with the variants.
Krishna Udayakumar, the founding director of the Duke Global Health Innovation Center, says due to the emerging mutants, we will likely need boosters or vaccine updates for years to come. On Tuesday, the New York City health department released its first detailed report on surveillance for the B.1.1.7 variant, the one originally identified in the U.K. It now makes up six percent of new COVID-19 cases. That’s up from 2.7 percent in January, backing original predictions that this more transmissible and potentially deadlier mutant would double every 10 days. Long Island this week also reported the state’s first case of the B.1.351 strain, which hails from South Africa and can partially bypass immunity.
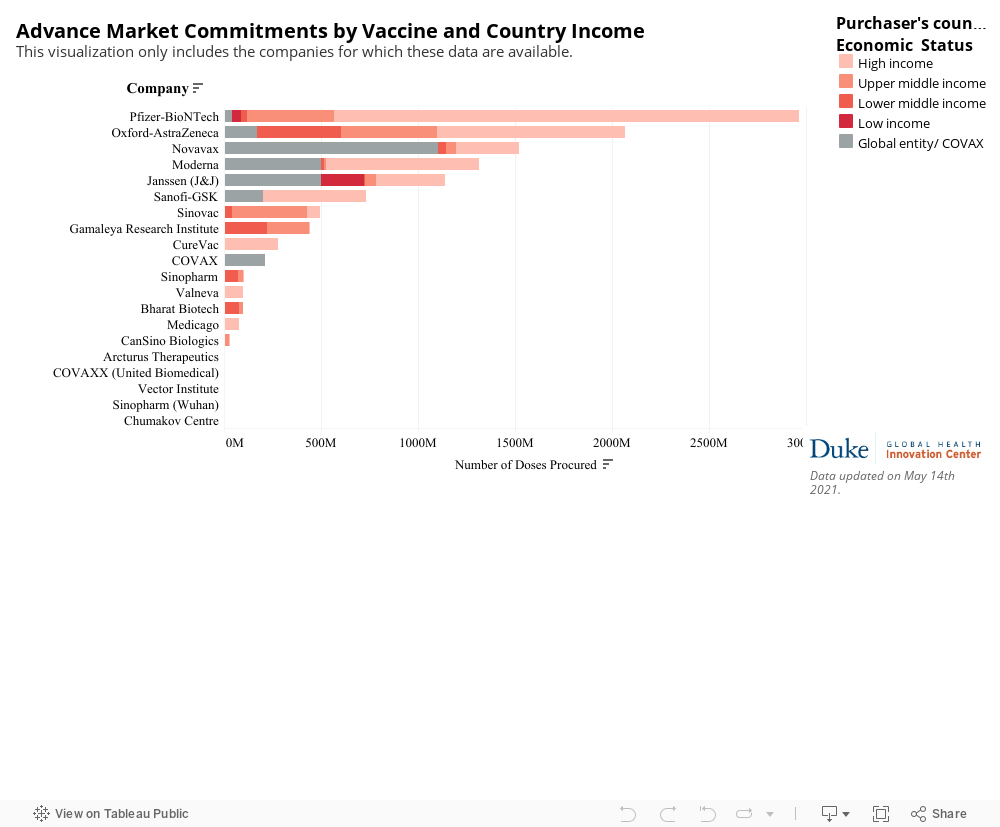
That means we need to exponentially increase our vaccine supply: Currently, many countries don’t expect to receive vaccines to be widely available until 2022 at the earliest. The World Health Organization has created the COVAX initiative to share vaccines globally, and the Biden administration recently pledged $4 billion, although it has not committed to sharing doses. Twenty-two high-income nations, including the U.S., possess more than half of the confirmed supply of COVID-19 vaccines.
Udayakumar argues that global distribution also needs to be equitable.
“If only rich and powerful people in low-income countries get access, that doesn’t improve equity,” Udayakumar said. “We wasted too much of the first year figuring out what needed to happen...We can’t get it wrong going forward.”




